For patients with Primary Biliary Cholangitis (PBC):
dynamic pbc landscape

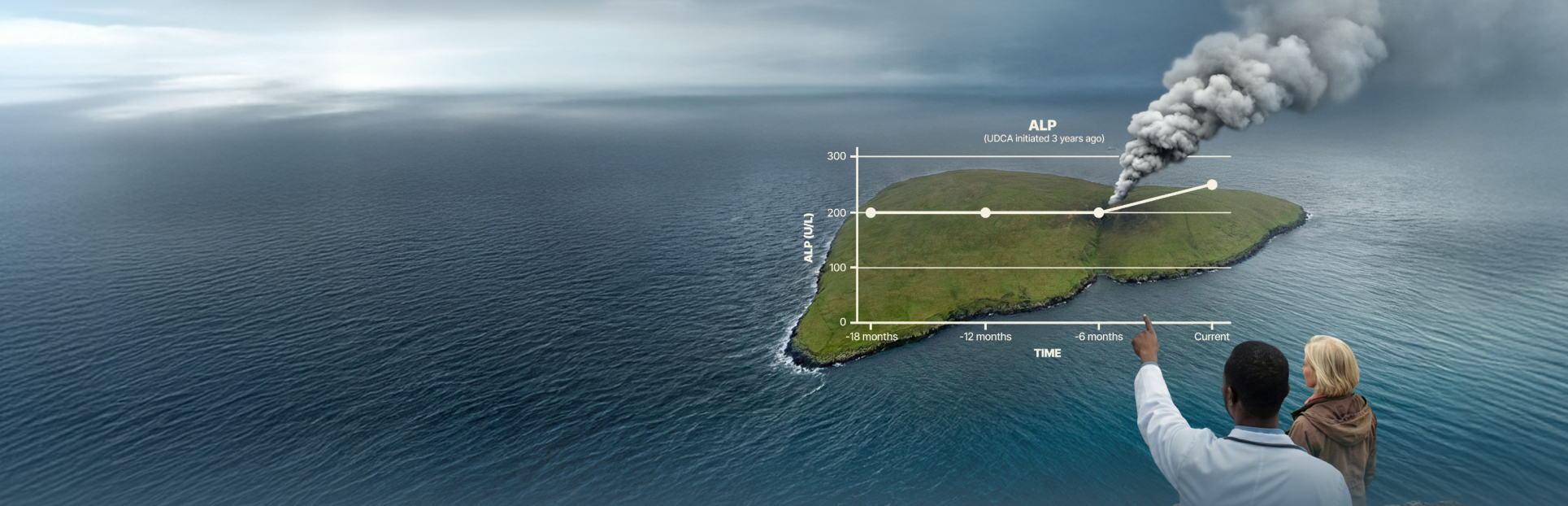
Once Alp Rises,
how has the landscape of your patient’s physiology changed?
ALP is an early, gold-standard indicator of cholestatic activity1,6
In Primary Biliary Cholangitis (PBC), cholestasis stimulates increased production of ALP by hepatocytes and cholangiocytes and causes ALP release into the serum.1,7
As cholestatic stress builds, the physiologic landscape continues to change
and alp rises in response1,4
ALP=alkaline phosphatase.
Switch between tabs
to see the Cycle of Pathogenesis and how UDCA can impact that cycle.
Rising ALP can signal physiological damage
already smoldering beneath the surface1-4

Bile acid accumulation drives hepatocellular stress,
increasing ALP production and release1,3,4,8
for pbc, udca monotherapy is
the standard of care in first-line1
The presence of UDCA can improve bile flow, reducing bile acid cellular toxicity1

While UDCA is effective,
some patients can progress at some point9*
*Study included a review of 1615 patients with early stage PBC with a median follow-up time of 7.9 years. 88% of patients were receiving UDCA treatment.9
UDCA=ursodeoxycholic acid

RISING ALP IS THE ALERT
that physiology may be Changing and action should be taken1,4,5,10
diverging physiology
~1 in 2 patients with early stage pbc advance to a more severe biochemical stage
within 5 years on udca therapy9*
See what can fuel progression in one patient, while the other remains relatively stable
Patients like Jan and Sara, who share the same diagnosis and therapy, can look very similar on paper. But over time, their disease courses can diverge. One of these women living with PBC will have disease progression, rising ALP could have been used as a signal to detect potential underlying physiologic changes early.1,3-5,8
*Study included a review of 1615 patients with early stage PBC with a median follow-up time of 7.9 years. 88% of patients were receiving UDCA treatment.9


As the inflection point is crossed, progression intensifies1,11

The difference between a stable patient and one whose disease progression intensifies is that
the persistence of immune-driven bile duct injury has crossed an inflection point1,11
changing trajectory
Even subtle, prolonged rises in ALP can
fuel the risk of serious outcomes13
A retrospective cohort study (n=3974) of PBC patients was conducted using Komodo's Healthcare Map, which is derived primarily from claims data. The overall median follow-up time was 2.5 years, during which 75.0% of patients received UDCA.13
Prolonged elevation of multiple hepatic biomarkers and fibrosis scores is associated with a greater risk of negative clinical outcomes, underscoring the importance of ongoing monitoring to help improve PBC management.13
ALP ≥ ULN
for 3 years
~70%
Increased Risk
A patient with an elevation of ALP ≥ ULN for 3 years had a 71.0% increased risk of negative outcomes13

ALP ≥ ULN &
TB ≥ 0.6 x ULN
for 3 years
~3x
greater Risk
When ALP ≥ ULN was combined with a TB ≥ 0.6 x ULN for 3 years, the risk of these negative outcomes was 2.89-fold greater than in a patient who never exceeded these thresholds13
Manage the risk early
AASLD and EASL PBC guidelines reinforce reading the landscape early with proactive management. Recommendations include1,5:
monitor liver labs frequently (Every 3-6 months)5
Regular, proactive monitoring helps detect patients who are inadequate responders to UDCA after 12 months of therapy.5
Confirming appropriate udca dosing (13‑15 mg/kg/day)5
An optimal dose of 13 to 15 mg/kg/day is correlated with improved biochemical response and survival.5
routinely discussing management approaches WITH YOUR PATIENT1
Consider structured life-long follow-up for your patients, as they have different disease courses, and may require varied levels of attention.1
AASLD=American Association for the Study of Liver Diseases; EASL=European Association for the Study of the Liver.
What matters
when the smoke rises
When ALP rises, here’s what to keep in mind:
PHYSIOLOGY CHANGES
When ALP rises, it can signal an inflection point, marking a potential physiologic change within your patient.1-4
TRAJECTORY SHIFTS
These physiologic changes can put patients on a different trajectory, increasing their risk of serious outcomes13
CONSIDER INCREASING MONITORING FREQUENCY
Rising ALP can lead to long-term negative outcomes, so more frequent monitoring can help you detect the early signs of hepatocellular stress1,2,5,13

keep the conversation going
References
1. Hirschfield GM, Beuers U, Corpechot C, et al. EASL Clinical Practice Guidelines: The diagnosis and management of patients with primary biliary cholangitis. Journal of Hepatology. 2017;67(1):145-172. doi:10.1016/j.jhep.2017.03.022 2. Tanaka A, Ma X, Takahashi A, Vierling JM. Primary biliary cholangitis. The Lancet. 2024;404(10457):1053-1066. doi:10.1016/S0140-6736(24)01303-5 3. Suzuki N, Irie M, Iwata K, et al. Altered expression of alkaline phosphatase (ALP) in the liver of primary biliary cirrhosis (PBC) patients. Hepatology Research. 2006;35(1):37-44. doi:10.1016/j.hepres.2006.01.009 4. Poupon R. Liver alkaline phosphatase: A missing link between choleresis and biliary inflammation. Hepatology. 2015;61(6):2080-2090. doi:10.1002/hep.27715 5. Lindor KD, Bowlus CL, Boyer J, Levy C, Mayo M. Primary Biliary Cholangitis: 2018 Practice Guidance from the American Association for the Study of Liver Diseases. Hepatology. 2019;69(1):394-419. doi:10.1002/hep.30145 6. Corpechot C, Carrat F, Poujol-Robert A, et al. Noninvasive elastography-based assessment of liver fibrosis progression and prognosis in primary biliary cirrhosis. Hepatology. 2012;56(1):198-208. doi:10.1002/hep.25599 7. Carbone M, Milani C, Gerussi A, et al. Primary biliary cholangitis: a multifaceted pathogenesis with potential therapeutic targets. Journal of Hepatology. 2020;73(4):965-966. doi:10.1016/j.jhep.2020.05.041 8. Hatoff DE, Hardison WG. Induced synthesis of alkaline phosphatase by bile acids in rat liver cell culture. Gastroenterology. 1979;77(5):1062-1067. 9. Gatselis NK, Goet JC, Zachou K, et al. Factors Associated With Progression and Outcomes of Early Stage Primary Biliary Cholangitis. Clinical Gastroenterology and Hepatology. 2020;18(3):684-692.e6. doi:10.1016/j.cgh.2019.08.013 10. Romeo M, Di Nardo F, Basile C, et al. The Personalized Management of Primary Biliary Cholangitis in the Era of Precision Medicine: Current Challenges and Future Perspectives. J Pers Med. 2025;15(12):597. Published 2025 Dec 3. doi:10.3390/jpm15120597 11. Jones D, Boudes PF, Swain MG, et al. Seladelpar (MBX-8025), a selective PPAR-δ agonist, in patients with primary biliary cholangitis with an inadequate response to ursodeoxycholic acid: a double-blind, randomised, placebo-controlled, phase 2, proof-of-concept study. The Lancet Gastroenterology & Hepatology. 2017;2(10):716-726. doi:10.1016/S2468-1253(17)30246-7 12. Del Barrio M, Díaz-González Á, Alonso-Peña M. Primary Biliary Cholangitis: Immunopathogenesis and the Role of Bile Acid Metabolism in Disease Progression. IJMS. 2025;26(16):7905. doi:10.3390/ijms26167905 13. Kowdley KV, Victor DW, MacEwan JP, et al. Longitudinal Relationship Between Elevated Liver Biochemical Tests and Negative Clinical Outcomes in Primary Biliary Cholangitis: A Population‐Based Study. Aliment Pharmacol Ther. 2025;61(11):1775-1784. doi:10.1111/apt.70120